



IBS Symptoms & Its SubTypes
Most children with ASD also suffer from IBS Symptoms at some stage. IBS or Irritable Bowel Syndrome is a common gastrointestinal condition affecting up to 40% of adults (5-20% of men and 15-25% of women).
The main gastrointestinal symptoms of IBS are chronic or recurrent abdominal pain or discomfort, associated with changes in bowel habits (e.g., diarrhoea and/or constipation).
Common IBS Symptoms
Symptoms that cumulatively support the diagnosis of IBS-
- Abnormal stool frequency (e.g., more than 3 bowel movements per day or less than 3 bowel movements per week).
- Abnormal stool form (lumpy/hard or loose/watery).
- Abnormal stool passage (straining, urgency, feeling of incomplete evacuation).
- Passage of mucus.
- Bloating or feeling of abdominal distension.
IBS Affects More Women Than Men
The UNC Centre for Functional GI & Motility Disorders: National Survey of the Effects of Changes in Female Sex Hormones on Irritable Bowel Symptoms found the following:
- Women are 2-3 times more likely to suffer from IBS than men.
- Among women, IBS is most prevalent during the menstruation years.
- Over 50% of women seeing a gynecologist for lower abdominal pain have IBS.
- Women with IBS are 3 times more likely to undergo a hysterectomy than those without IBS.
- Women with IBS are more likely to be diagnosed with endometriosis than women with other bowel symptoms, suggesting the possibility of a common denominator.
- Over 60% of patients with IBS report rheumatological symptoms, such as skin rashes, muscle spasms, headaches, muscle aches, or Fibromyalgia.
IBS Symptoms in Females
- Menstruation is associated with exacerbation of IBS symptoms in most women with IBS.
- Pregnancy appears to improve IBS symptoms temporarily for many women.
- Oral estrogen and progesterone supplements do not seem to effect IBSsymptom severity.
- Hysterectomy or tubal ligation do not seem to effect IBS symptom severity.
- Endometriosis increases IBS bloating symptoms, but not others.
Rome IV Criteria for IBS
The Rome IV criteria is used for diagnosing IBS. Rome IV divides IBS into two major categories. In our experience, having assessed hundreds of faecal microbiology profiles, these two presentations are associated with different imbalances in intestinal bacteria. The difference can only be identified by a Faecal Microbiology Analysis from Bioscreen Medical. Bioscreen is one of the only commercial labs that refrigerates the faecal sample and transports it in an anaerobic (oxygen free) chamber prior to culturing analysis. They have developed a technique for growing, counting, and identifying the main species of Aerobic and Anaerobic gut bacteria that normally reside in the human gut (commensal bacteria).
Recurrent abdominal pain, on average, at least 1 day/week in the last 3 months, associated with two or more of the following:
- Related to defecation.
- Associated with a change in frequency of stool.
- Associated with a change in form (appearance) of stool.
- Criteria fulfilled for the last 3 months with symptom onset at least 6 months before diagnosis.
Subtypes of IBS
The four subtypes of IBS are described below:
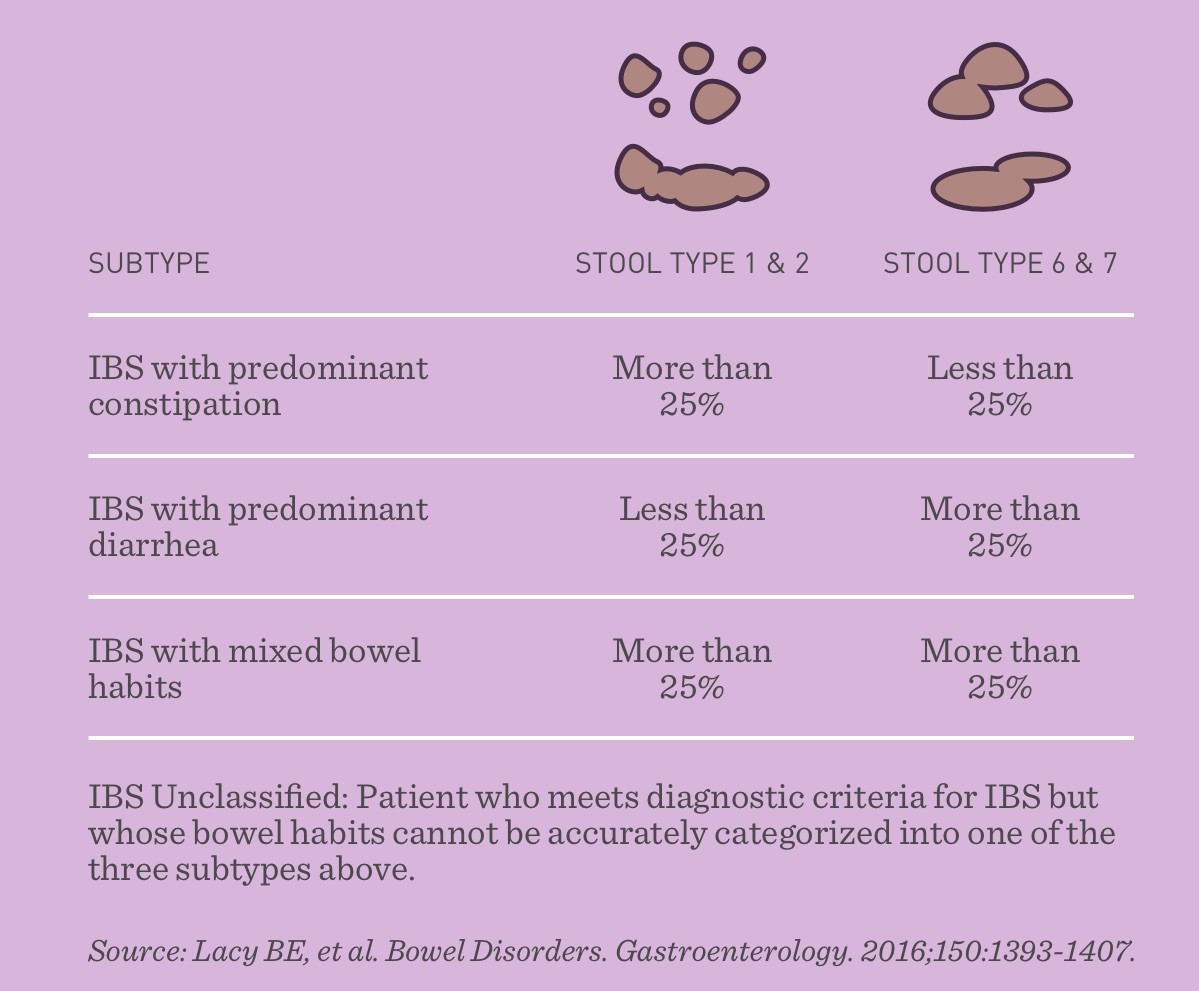
- IBS-C (predominant constipation)
- IBS-D (predominant diarrhoea)
- IBS-M (IBS with mixed bowel habits)
- IBS-U (people whose symptoms do not fit into any category are considered to have IBS unclassified)
IBS-C: Predominant Constipation
-
Symptoms tend to alternate between constipation and normal stools.
-
Symptoms of cramping pain in the lower abdomen (commonly triggered by eating).
This profile is more likely to be associated with a low E-Coli count in the faecal analysis. We understand that this is due to the E-Coli producing the amino acid Tryptophan which is a precursor to the brain’s neurotransmitter Serotonin. Serotonin is not only the ‘feel good’ neurotransmitter but is also essential to the initiation and maintenance of the peristaltic activity responsible for good gut motility.
Sugar and refined carbohydrates are easily fermented and converted to lactic acid. If a diet contains them in excess, it inhibits the growth and motility of E-coli which promotes the growth of Streptococcus and Bifidobacteria.
IBS-D: Predominant Diarrhoea
- The person may experience diarrhoea early in the morning or after eating.
- The need to empty the bowel is typically urgentand cannot be delayed.
- Incontinence problems can also co-occur.
IBS-M: IBS with Mixed Bowel Habits
- Symptoms vary between diarrhoea or loose stools, normal stools, and constipation.
IBS-U: Unclassified Category
This category includes people with some IBS symptoms who do not fit into the first three categories.
IBS & Work Disruption
- Studies indicate that, annually, people with IBS miss 3-4 times more workdays per year than the US national average of 5 days. This makes IBS one of the most common reasons for work or school absenteeism, second only to the common cold.
Risk Factors for IBS
Among women in a referral-based gastroenterology clinic:
- 51% reported a history of sexual and/or life-threatening physical abuse.
- Patients with functional disorders (e.g., IBS and unexplained abdominal pain) had experienced rape and life-threatening physical violence.
IBS Patients With An Abuse History (Compared to Patients Who Had Not Suffered Abuse)
- Had, on average, three medical symptoms (e.g., pelvic pain, headaches, genitourinary complaints, shortness of breath).
- Reported greater pain.
- Had twice the number of days spent in bed due to the illness.
- Had more functional disabilities (in the areas of work, self-care and psychosocial).
- Experienced more psychological distress.